50 Nursing Interview Questions and Answers (2026)

You spent years in school. You passed the NCLEX. You survived clinicals.
And now there's a 45-minute interview standing between you and the job.
Nursing interviews are not like other job interviews. The hiring manager isn't just checking if you're a good communicator. They're checking whether you think like a safe nurse. Every "tell me about a difficult situation" question is really a test of your clinical judgment. Every "tell me about yourself" is a chance to connect who you are to why patient care matters to you.
This post covers the 50 questions that come up most often — across all units and experience levels. We grouped them by category, wrote full model answers for the most important ones, and added the key points you need to hit for the rest.
Why nursing interviews are different
In most job interviews, behavioral questions are a formality. In nursing, they're the whole game.
When a nurse manager asks "tell me about a time a patient deteriorated unexpectedly," she's not making small talk. She's checking whether you recognized the warning signs, escalated at the right time, and communicated clearly under pressure. Your answer reveals how you think clinically — more than any resume bullet ever could.
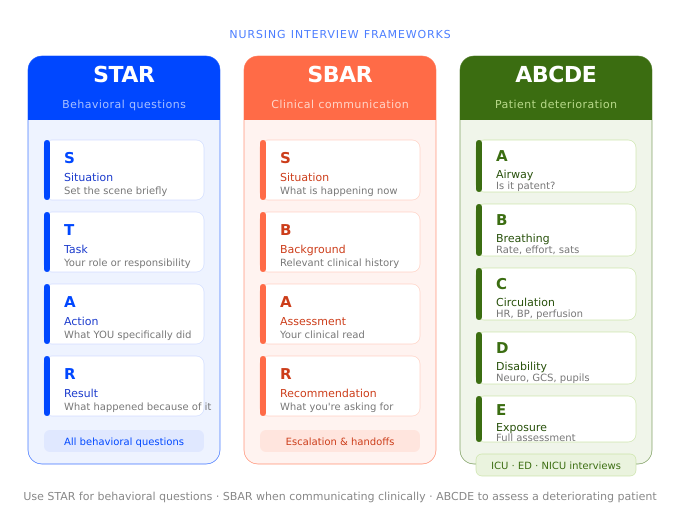
This is why two frameworks come up over and over in strong nursing answers:
STAR — Situation, Task, Action, Result. Use this for behavioral questions about conflict, teamwork, mistakes, and going above and beyond.
SBAR — Situation, Background, Assessment, Recommendation. Use this for anything involving clinical communication: calling a physician, escalating a concern, handing off a patient.
For high-acuity units like the ICU and ED, there's a third framework — ABCDE (Airway, Breathing, Circulation, Disability, Exposure) — that comes up in clinical scenario questions. We cover it in detail in the ICU and ED sections below, where it actually belongs.
You don't need to name the frameworks out loud in your answer. Just use the structure — the interviewer will notice.
Category 1: The Big 5 — Foundational Questions
These five questions show up in nearly every nursing interview, regardless of unit, hospital, or experience level. They feel easy, so most nurses underprepare them. Don't.
The questions:
- Tell me about yourself.
- Why did you choose nursing?
- Why do you want to work at this hospital?
- What are your biggest strengths and weaknesses?
- Where do you see yourself in five years?
Question 1: "Tell me about yourself."
This is almost always the opening question. Most nurses answer it like a resume walkthrough — "I went to X school, graduated in Y, did my clinicals at Z." That's not an answer. That's a LinkedIn profile read out loud.
A strong answer connects your background to your clinical values in about 90 seconds. Here's what that looks like:
"I'm a recent nursing graduate from [University Name]. During my senior year, I did most of my clinical hours on a busy med-surg floor and a six-week rotation in the ICU, which honestly changed how I think about nursing. Watching how the ICU nurses managed rapid deteriorations — staying calm, communicating clearly, always one step ahead — made me realize that's the kind of nurse I want to become.
Before nursing school I worked as a patient care tech for two years, so I've seen what the floor actually looks like when staffing is short and the census is high. I don't come in expecting a perfect environment. I come in ready to work, ready to ask questions when I'm unsure, and ready to grow.
I applied to [Hospital Name] specifically because of your new grad residency program and the mentorship I've heard about from nurses who trained here. I want to start somewhere I can build the right habits early."
Why this works: It connects real experience to clinical motivation. It acknowledges what floor nursing is actually like without complaining. It explains why this hospital specifically — which shows you did your homework. And it ends on learning, which is what every manager wants to hear from a new grad.
What NOT to say: Don't start with "I've always wanted to help people." Every single candidate says it. It tells the interviewer nothing about how you think.
Questions 2–5: Key points to hit
"Why did you choose nursing?"
- Tie it to a specific moment or experience, not a general feeling
- If a patient or family experience shaped your view of healthcare, this is the place to share it briefly
- Avoid: "I want to make a difference" (too vague) and "the job security" (true, but not what they want to hear)
"Why do you want to work at this hospital?"
- Research the hospital before you show up — Magnet status, residency structure, unit reputation, recent expansions
- Name something specific: "your level-one trauma designation" or "the new grad residency program" land better than "great reputation"
- Avoid: Answers that could apply to any hospital in the city
"What are your biggest strengths and weaknesses?"
- Strengths: Pick one that's clinically relevant. "I'm very careful about medication reconciliation" beats "I'm a hard worker"
- Weakness: Pick something real that you're actively working on. "I sometimes struggle to delegate because I want to make sure everything is done right — I've been working on trusting my team more" is honest and shows self-awareness
- Avoid: "I work too hard" as your weakness — every manager has heard it and no one believes it
"Where do you see yourself in five years?"
- Be honest about growth without making it sound like you're planning to leave in six months
- "I want to become a strong bedside RN first, then explore a critical care certification" shows direction without locking you in
- For new grads: mentioning a specialty you're drawn to shows ambition without sounding unrealistic
Category 2: Behavioral Questions — The STAR Method
Behavioral questions always start with "tell me about a time…" They're the core of most nursing interviews because past behavior is the best predictor of future behavior.
The STAR method gives your answer a clear shape:
- Situation — set the scene briefly
- Task — what was your role or responsibility
- Action — what did you specifically do
- Result — what happened because of it
The key word is you. Hiring managers will push back if your answer keeps saying "we." They want to know what you did, not what the team did.
The questions:
- Tell me about a time you handled a difficult patient or family member.
- Describe a conflict you had with a coworker and how you resolved it.
- Tell me about a time you had to work under a lot of pressure.
- Give me an example of a time you went above and beyond for a patient.
- Tell me about a time you had to adapt quickly to an unexpected change.
- Describe a time you made a mistake. What did you learn from it?
- Tell me about a time you had to deliver bad news.
- Have you ever disagreed with a care decision? What did you do?
- Tell me about a time you had to prioritize multiple patients at once.
- Describe a situation where you had to advocate for a patient.
Question 6: "Tell me about a time you handled a difficult patient or family member."
"During my med-surg rotation, I had a patient in his 60s who was refusing to take his blood pressure medication. He was angry, told me it was making him feel worse, and asked me to leave the room.
Instead of escalating right away, I came back an hour later and just asked him to tell me more about what he was feeling. It turned out he was getting dizzy every time he stood up, and it was scaring him. Nobody had explained that orthostatic hypotension is a common side effect and something we could actually manage.
Once I explained what was happening and gave him a concrete plan — sit up slowly before standing, use the call button before getting out of bed — his attitude completely changed. He took his medication that day and every day after. I documented the conversation and flagged it to the charge nurse because it was relevant to his discharge plan.
He thanked me before he left the unit. That part I didn't expect."
Why this works: It shows clinical knowledge (orthostatic hypotension), communication skills, documentation, and judgment about when to escalate — all in one answer. The last line is human. Real nurses remember the moments that surprised them.
Questions 7–15: Key points to hit
Conflict with a coworker
- Show that you addressed it directly and professionally, not through gossip or avoidance
- "I asked if we could speak privately" signals maturity
- Avoid making your coworker the villain — interviewers know there are always two sides
Working under pressure
- Be specific about what the pressure was: short staff, multiple deteriorating patients, a code
- Show how you organized yourself, not just that you got through it
- Mention how you communicated with the team as things escalated
Going above and beyond
- Keep it patient-centered, not self-congratulatory
- Small, genuine moments often land better than dramatic ones
Adapting to unexpected change
- Charge nurses love this question — it reveals whether you panic or pivot
- Show that you communicated the change to the people who needed to know
Making a mistake (Question 11 — the general behavioral version)
This version shows up in standard behavioral rounds and applies to any nursing role. It doesn't have to be a clinical error — it can be a communication failure, a missed handoff detail, or a judgment call that didn't go the way you expected. The key is accountability and what you changed. (Note: ICU and ED interviews often ask a more specific version of this question focused on clinical errors — see Question 18 in Category 3.)
- You must answer this honestly. Saying "I can't think of one" is a red flag
- Show accountability, what you changed, and what the outcome was
- Avoid picking a mistake with serious patient harm if you have another option — pick one that shows genuine growth
"During my clinical rotation on a med-surg floor, I was caring for a patient who had just returned from a procedure. She mentioned she was feeling nauseous, and I noted it but didn't follow up as quickly as I should have — I got pulled into another patient's room and assumed it was procedure-related and would pass.
About an hour later, a more experienced nurse noticed the patient had barely moved and her color wasn't great. We reassessed together and found her blood pressure had dropped. She ended up being fine, but it required intervention that could have happened sooner.
I've thought about that shift a lot. What I changed: I now do a 30-minute check-in after any patient returns from a procedure, even when I'm busy. I write it on my assignment sheet so I don't rely on memory. It's a small habit, but it came from a real lesson."
Why this works: It's honest without being catastrophic. It shows clinical self-awareness. And the specific behavioral change at the end — writing it on the assignment sheet — is concrete and believable.
Disagreeing with a care decision
- Different from the physician disagreement question in Category 3 — this can be about a care plan, discharge timing, or a team decision
- Show that you raised the concern the right way, through the right channel
Prioritizing multiple patients
- Walk through ABC priorities, time-sensitive medications, safety risks
- Show your thinking process, not just what you decided
Patient advocacy
- The strongest answers involve speaking up when something felt wrong, even when it was uncomfortable to do so
- Family communication, care transitions, and discharge planning are all common settings for this
Category 3: Clinical Questions — Patient Safety and SBAR
This is where nursing interviews separate from every other job interview in the world.
Hiring managers for clinical roles — especially in the ICU, ED, and NICU — use these questions to assess whether you can think safely under pressure. A weak answer here ends an interview faster than anything in the previous two categories.
The single most important thing to understand: safety comes first in every clinical answer. Before calling anyone, before updating the family, before anything — your first move was to make sure the patient was safe. If your answer doesn't make that clear, the interviewer will notice.
The questions:
- Tell me about a time a patient deteriorated unexpectedly. What did you do?
- How do you prioritize when two patients need you at the same time?
- Tell me about a time you made a clinical mistake and what you learned.
- Have you ever disagreed with a physician about a patient's care? What happened?
- How do you use SBAR in your clinical practice?
- Describe your approach to a patient who is deteriorating.
- What would you do if you found a medication error that a previous nurse made?
- Tell me about a time you had to escalate a concern to a physician or charge nurse.
- How do you ensure safe patient handoffs?
- What do you do when you're unsure about a clinical decision?
Question 18: "Tell me about a time you made a clinical mistake."
This is not the same question as Question 11. In behavioral rounds, any meaningful mistake works — a communication failure, a missed handoff detail, a judgment call that went wrong. In ICU, ED, and NICU interviews, the word clinical is doing real work. They want a patient-care scenario: a missed assessment finding, a delayed escalation, a lab value you didn't act on quickly enough. A general workplace mistake won't satisfy this question.
What they're actually testing: whether you have the self-awareness to identify what you missed clinically and the judgment to change your practice because of it.
"During my ICU rotation, I was monitoring a post-op patient who had been stable all shift. Around hour six, he mentioned he felt a little off — just tired, he said. I noted it, assumed it was normal post-op fatigue, and moved on to my other patient.
About 40 minutes later his nurse came back to check vitals and his lactate had been trending up on the last draw. We escalated quickly, but looking back, I had a window earlier where his symptoms plus the lactate trend should have prompted me to reassess sooner.
What I changed: I now treat 'I just feel off' as a clinical data point, not small talk. I also started doing a quick mental recap at the start of every hour — what did each patient tell me, and does anything they said warrant a second look? It sounds simple, but that habit came directly from that shift."
Why this works: It names a specific clinical signal that was underweighted (patient-reported symptom plus a rising lactate trend). It doesn't catastrophize — the patient was escalated and managed. And the behavioral change is concrete and believable, not a vague "I'll be more careful next time."
What NOT to say: Anything that suggests you've never made a clinical error, or that the mistake was really someone else's fault. ICU and ED managers have heard every deflection. Accountability is the whole point of the question.
Question 19: "Have you ever disagreed with a physician about a patient's care?"
This question is asked in almost every RN interview. The hiring manager is checking three things at once: whether you can advocate for your patient, whether you know the right channels to do it, and whether you can stay professional when you're scared or frustrated.
"During my ICU rotation, I was caring for a post-op patient who I felt was showing early signs of respiratory distress. Her oxygen saturation was trending down, her respiratory rate had climbed, and she was more agitated than she'd been an hour earlier. The covering physician had already assessed her and felt she was stable — just anxious.
I wasn't comfortable with that assessment. I went back to him and used SBAR to walk through exactly what I was seeing: her sats had dropped from 97 to 93 over two hours, her respiratory rate had gone from 18 to 26, and she was now using accessory muscles. I asked specifically whether we should get an ABG or consider increasing her oxygen support.
He came back to reassess, ordered the ABG, and the results showed early respiratory acidosis. We ended up transferring her to a higher level of care.
Afterward I talked to my preceptor — not to get credit, but because I wanted to know if I'd handled the escalation the right way. She said I had. Going back with specific data instead of just repeating my concern made the difference."
Why this works: It uses SBAR clearly. The concern is backed by clinical data, not just a gut feeling. It goes through the right channel. And the conversation with the preceptor at the end shows self-reflection rather than ego.
What NOT to say: "I would just follow the doctor's orders." This is the most common wrong answer to this question and it fails the patient advocacy test every time. Hiring managers notice it immediately.
The Clinical Safety Signal
In any clinical scenario question, the first thing your answer should communicate is that the patient was safe. Hiring managers in the ICU, ED, and NICU are listening for this before anything else. If your answer starts with "I called the doctor first" — that's a problem. Assess the patient, stabilize what you can, then communicate.
Questions 16–25: Key points to hit
Patient deterioration
- Walk through your assessment in order: airway, breathing, circulation — and ABCDE for ICU/ED
- Always mention that you stayed with the patient or made sure someone else did
- Escalation timing matters — show you didn't wait too long
Prioritizing two critical patients
- Walk through your thinking: who has the more time-sensitive need, who can safely wait two minutes, how you looped in the charge nurse
- There's no single right answer — they want to see your reasoning
Finding a medication error
- Assess the patient first, always
- Follow your facility's incident reporting process
- Never cover for another nurse — it's a patient safety issue, not a loyalty issue
SBAR in practice
- If you're a new grad who hasn't used it in real practice yet, say "in simulation and during clinicals, I practiced..." — don't pretend to have years of experience you don't have
- Know the structure cold: what you're calling about, relevant background, your assessment, what you're asking the physician to do
Escalating a concern
- Lead with specific data, not just a feeling
- Early escalation is always better — show you didn't wait until things were critical
Safe handoffs
- SBAR is standard, and some programs also teach I-PASS
- Always verify: active drips, pending labs, outstanding patient or family concerns
When you're unsure
- "I look it up, I ask my charge nurse, I call pharmacy" — knowing your resources is a sign of good judgment, not weakness
- Never guess on a clinical decision
Category 4: Specialty-Specific Questions
A note for nurses leaving bedside care
If you're moving away from bedside nursing — into case management, a clinic, insurance, education, or an outpatient setting — you'll face a different kind of interview challenge. The questions aren't harder, but they require you to reframe bedside skills in a new context.
Hiring managers in these roles want to know that you can translate what you did at the bedside into the new setting. "I managed six patients per shift" becomes "I'm comfortable managing high volumes and shifting priorities quickly." "I escalated clinical concerns daily" becomes "I know how to identify problems early and communicate them to the right people."
The most common mistake in these interviews is underselling your bedside experience because you assume it doesn't apply. It does. A nurse who has worked a busy med-surg floor for three years has more real-world communication, prioritization, and crisis management experience than most non-clinical candidates could ever demonstrate. Frame it that way.

New Grad RN
If you're a new grad, the interviewer knows you don't have years of independent practice. They're not looking for a veteran. They're looking for someone who knows what they don't know — and knows how to find out.
The questions:
- What do you feel least prepared for as a new nurse?
- Tell me about a clinical situation from your rotations that challenged you.
- How do you handle feedback or criticism from a more experienced nurse?
- What would you do if you weren't sure whether to administer a medication?
- How do you plan to manage the transition from student to staff nurse?
Key points:
- Question 26: Be honest. "I know managing a full patient load is going to be a learning curve — I've never been responsible for more than three patients at once" is a stronger answer than pretending you're ready for anything. Follow it with how you're planning to close that gap.
- Question 27: Pick something that shows clinical reasoning, even if the outcome wasn't perfect. Learning from it matters more than getting it right the first time.
- Question 28: Show that you're coachable. New grads who get defensive about feedback are a red flag on any unit.
- Question 29: "I would hold the medication, look it up, and verify with my charge nurse or pharmacist before giving it." Always. Never guess.
- Question 30: Talk about using your preceptor fully, asking questions before you need to, and not letting pride get in the way of safe care.
ICU / Critical Care
ICU interviews go deep on clinical knowledge, fast decision-making, and your ability to manage complex patients with multiple moving parts. If you haven't worked in an ICU yet, lean on rotation experience, simulation, or your NCLEX prep — and be honest about where your gaps are.
The questions:
- How do you assess a patient who is rapidly deteriorating?
- Walk me through how you would respond to a patient going into respiratory failure.
- Tell me about your experience with vasoactive drips or ventilator management.
- How do you manage a high-acuity patient load while keeping all patients safe?
- What does your rapid response process look like?
Key points:
- Question 31: This is where the ABCDE framework belongs. Airway → Breathing → Circulation → Disability (neuro status) → Exposure. This is the standard rapid assessment order used in critical care and emergency settings. Walking through your answer in this order signals to the interviewer that your clinical thinking is structured, not reactive. Commit this to memory before the interview.
- Question 32: Call for help early. In any near-code situation, you are never supposed to manage it alone. Knowing when to escalate is more impressive than claiming you'd handle it solo.
- Question 33: If your experience is limited, say so and explain what you've done to learn. "I haven't managed a norepinephrine drip independently yet, but during my ICU rotation I spent time with the pharmacist understanding how vasopressors work and what to watch for" is an honest answer that still shows initiative.
- Question 34: Prioritization and communication. What's time-sensitive right now? What can safely wait 15 minutes? Who needs to know what?
- Question 35: Know the general structure of rapid response teams. If you're unfamiliar with theirs specifically, say what you've been taught and ask how it works at their facility — interviewers respect candidates who ask smart follow-up questions.
Emergency Department
ED interviews focus on your ability to make fast decisions with incomplete information, stay organized in chaos, and triage accurately when multiple patients arrive at once.
The questions:
- How do you approach triage when three patients arrive at the same time?
- Tell me about a time you made a fast decision with limited information.
- How do you manage a patient who is agitated or combative?
- What's your approach when a patient is crashing and the attending isn't immediately available?
- How do you stay organized during a high-volume shift?
Key points:
- Question 36: Walk through triage logic: life-threatening first, then urgent, then less urgent. If you've been trained on ESI (Emergency Severity Index) levels, reference them here.
- Question 37: Show that you gathered what data you could, made a decision, and then reassessed. Freezing up is dangerous in the ED.
- Question 38: De-escalation first. Show you know verbal tools before reaching for pharmacological or physical interventions. "I approach calmly, introduce myself, and try to understand what's driving the agitation" before calling for backup.
- Question 39: Start your ABCDE assessment (Airway → Breathing → Circulation → Disability → Exposure), activate help, and don't wait for the attending to begin. They'll catch up.
- Question 40: Talk through how you track your patients and communicate when things get busy. Systems matter more than stamina in the ED.
Med-Surg
Med-surg nurses manage the widest variety of patients in any hospital unit. Interviews here focus on time management, organization, and the ability to spot when a "stable" patient is becoming unstable.
The questions:
- How do you manage a five- or six-patient assignment when everyone seems to need you at once?
- Tell me about a patient you were worried about who ended up being more unstable than they first appeared.
- How do you handle end-of-shift handoff when you're behind on documentation?
- How do you approach discharge planning as part of daily care?
- What do you do when a patient's condition changes and the physician is hard to reach?
Key points:
- Question 41: Show your prioritization system. Time-sensitive medications and safety checks first, then assessments in order of acuity. Use your charge nurse when you're stretched.
- Question 42: This is the early warning question in disguise. Show that you trusted your instinct, gathered data, and escalated before things got worse.
- Question 43: Safety-critical documentation first: assessments, medications given, any clinical events. Administrative documentation second. "I never leave something undocumented that the next nurse needs to safely care for this patient" is the right line.
- Question 44: Discharge planning starts on admission, not the morning of discharge. Who's going home? Where are they going? What do they need to understand? Who needs to be involved?
- Question 45: Work up the chain: charge nurse, rapid response team, on-call physician. Document every attempt.
Category 5: Soft Skills and Teamwork
These questions decide whether people actually want to work with you for 12 hours straight.
The questions:
- How do you handle a heavy workload without burning out?
- Tell me about a time you helped a struggling coworker.
- How do you approach patients from different cultural backgrounds?
- Describe a time you had to explain a complex medical situation in plain language to a patient or family.
- What does patient advocacy mean to you?
Key points:
Question 46 — Handling heavy workloads
- Show that you know your limits and that you ask for help before you're drowning
- "I'd rather ask for help at hour two than be unsafe at hour ten" is a strong, honest line
- Don't pretend you never struggle — everyone in nursing struggles
Question 47 — Helping a coworker
- Show that you noticed without being asked
- Small moments count: helping someone turn a patient, covering a break, jumping in on a discharge
- The best answers show a team culture you actively built, not just one you benefited from
"About two months into my first job, I noticed one of the newer nurses on my unit — she'd been there about three weeks — was getting really quiet around hour six of her shift. She wasn't asking for help but she also wasn't answering call lights as fast as usual, and I could see she had a lot of patients with high needs that day.
I finished my own assessments, then just walked over and asked if she wanted me to take one of her vitals rounds while she caught up on documentation. She looked almost relieved that someone had asked. We split a couple of tasks for about 20 minutes.
She told me later that she'd been close to crying in the med room. Nobody had noticed, or at least nobody had said anything. I didn't do anything dramatic — I just paid attention. That's what I think teamwork actually looks like most of the time."
Why this works: It's specific and unglamorous in the best way. It shows situational awareness, initiative, and a team mindset that doesn't need recognition. The closing line is the kind of thing a real nurse would say.
Question 48 — Cultural competency
- This is a real clinical skill, not a checkbox
- Show that you ask patients about their preferences rather than assuming
- Avoid: "I treat everyone equally" — equity in healthcare means meeting people where they are, which often looks different for different patients
Question 49 — Patient education
- Use a specific example. "I explained a new insulin regimen using a simple drawing, then had the patient teach it back to me before discharge" is a real answer
- The teach-back method is worth mentioning if you've used it — it signals that you verify understanding, not just that you talked
Question 50 — Patient advocacy
- This should feel personal to you, not like a definition you memorized
- The strongest answers are grounded in a specific moment — a time you spoke up for someone who couldn't speak for themselves
- "Advocacy means making sure a patient's voice is heard, even when they're scared or confused" is a start — but connect it to something real from your experience
Questions to Ask the Interviewer
Most nurses treat this part of the interview as optional. It isn't.
The questions you ask tell the hiring manager what kind of nurse you'll be. Generic questions ("what does a typical day look like?") suggest you didn't prepare. Specific, thoughtful questions signal that you've done your research and you care about the specifics of this unit — not just getting hired anywhere.
Here are five questions that consistently land well:
1. "What does your nurse-to-patient ratio look like on this unit, and does it change between day and night shifts?"
This shows that you understand staffing ratios are a patient safety issue, not just a scheduling preference.
2. "What does onboarding look like for a new hire — how long is orientation, and do I have a consistent preceptor throughout?"
For new grads especially, this matters a lot. A disorganized orientation is one of the top reasons new nurses leave their first job within a year.
3. "How does the team handle rapid responses — is there a dedicated rapid response team, or does the floor manage initially?"
A great question for any med-surg or step-down candidate. It shows that you're thinking about systems, not just individual practice.
4. "What's the biggest challenge nurses on this unit face right now?"
This opens up an honest conversation and you'll learn something real. Hiring managers remember candidates who ask this.
5. "What qualities do your most successful new hires have?"
Slightly bold, but it works. It gives you useful information you can reference in the rest of the interview, and it shows confidence.

Reading questions is a start. Practicing them is how you get hired.
Vorna asks you real nursing interview questions based on your resume and the job description you're applying for — then gives you a full feedback report on your answers. Free to start, no subscription.
Reading questions is one thing. Answering them out loud under pressure is another. Start your free practice interview on Vorna →