Nursing Behavioral Interview Questions and the STAR Method: A Practical Guide

Most nurses going into an interview have heard of the STAR method. They know the letters stand for something — Situation, Task, Action, Result — and they have a vague plan to "use it" when the behavioral questions come up.
Then the interviewer asks "tell me about a time you had to manage a really difficult patient," and the answer comes out as a three-minute story that never quite lands, jumps around in time, and ends with "so yeah, it worked out."
The STAR method is not magic. Knowing the framework does not automatically produce a good answer. What produces a good answer is understanding why the structure works, what each part is actually supposed to do, and how to apply it to clinical nursing scenarios specifically — not just generic job interview questions.
That's what this guide covers. We'll walk through the framework clearly, show you what each part looks like in a clinical nursing context, and give you model answers for the behavioral questions that come up most often in nursing interviews.
What the STAR Method Actually Is
STAR is a structure for answering behavioral interview questions — the ones that start with "tell me about a time..." or "describe a situation where..."
Here's what each letter does:
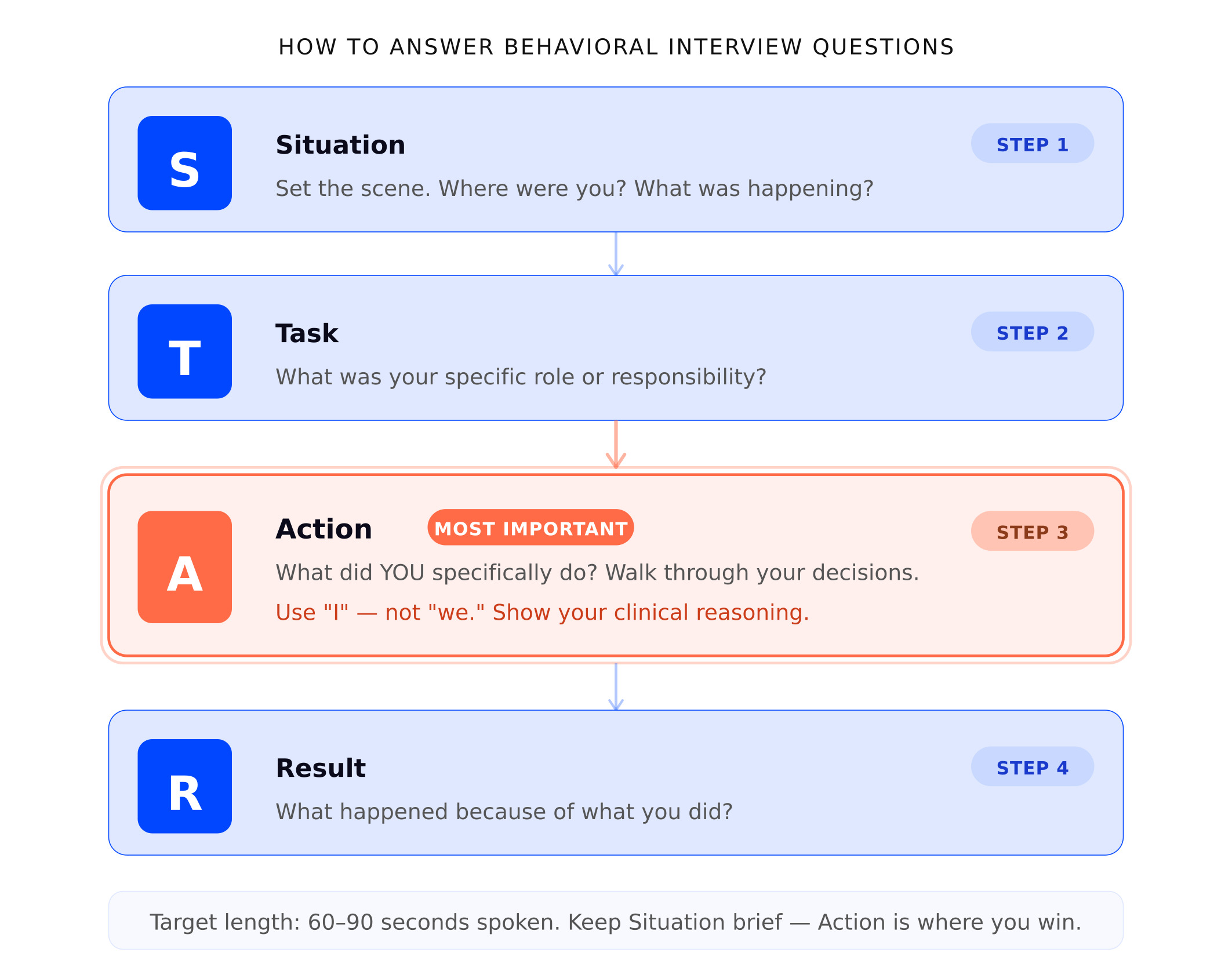
S — Situation. Set the scene. Give the interviewer just enough context to understand the circumstances. Where were you? What was the clinical setting? What was happening?
T — Task. What was your specific role or responsibility in that situation? What were you expected to do?
A — Action. What did you specifically do? This is the most important part of the answer. Walk through the steps you took, the decisions you made, the things you said.
R — Result. What happened because of what you did? What was the outcome for the patient, the team, or the situation?
The whole answer should take about 60 to 90 seconds when spoken out loud. Shorter than that and you haven't given enough detail. Longer and you're rambling past the point.
Why It Works — And Why Most Nurses Don't Use It Well
The STAR method works because it forces a clear beginning, middle, and end. It keeps you focused on specifics rather than generalities. And it answers the question an interviewer is actually asking, which is: what did you do in a real situation, and what happened as a result?
Here's the problem: most nurses either skip a step or weight them wrong.
The most common mistake is spending too long on the Situation and running out of time for the Action and Result. You set up the scenario in great detail — the unit, the patient, the shift — and then you rush through what actually happened because you've used most of your time. The Action is the part that matters most. The Situation is just context.
The second most common mistake is using "we" throughout the Action step. "We assessed the patient, we called the physician, we decided to escalate." The interviewer asked what you did. They know nursing is a team profession. But behavioral questions exist precisely to understand your individual judgment and contribution, not what the team did together. If you led the escalation, say that. If your preceptor made the final call, say that too — honesty about your role is not a weakness.
The third mistake is leaving out the Result. This happens when nurses are humble about outcomes, or when the outcome was messy and they feel uncomfortable claiming it. But the Result is what ties the story together. It doesn't have to be dramatic — "the patient stabilized and we were able to avoid a transfer to the ICU" is a perfectly good result. So is "the conflict with my coworker didn't fully resolve, but we were able to work together professionally after that conversation."
How STAR Works Differently in Nursing
In most job interviews, behavioral questions are about general professional skills — communication, collaboration, handling pressure. The STAR framework applies cleanly to those.
In nursing, behavioral questions are often doing double duty. On the surface, they're asking about your communication or teamwork. Underneath, they're testing your clinical judgment.
"Tell me about a time you had to prioritize multiple patients" is a STAR question. But the Action part of that answer needs to show clinical thinking — which patient had the most time-sensitive need, how you used your charge nurse, what you did to make sure nothing slipped. A generic "I stayed calm and got through it" answer fails the clinical test even if it technically follows the STAR structure.
This is why you can't just memorize a STAR story and plug it in. Your Action step needs to show that you think like a nurse, not just a professional who handled a stressful situation.
Whenever you write out a STAR story for a nursing interview, ask yourself: does the Action step show clinical reasoning? Does it show that patient safety was your first priority? Does it show that you communicated with the right people at the right time?
If the answer to all three is yes, you have a strong nursing STAR story.
The Most Common Nursing Behavioral Questions — With Model Answers
"Tell me about a time you handled a difficult patient or family member."
This question shows up in almost every nursing interview. It tests your communication skills, your patience, and your ability to stay professional when someone is scared, angry, or unreasonable.
The trap is framing the patient or family member as the problem. Even if they were difficult, your answer should show empathy and curiosity first — not frustration.
"During my med-surg rotation, I had a patient in his late fifties who was refusing his blood pressure medication every shift. He was dismissive and a little hostile about it — told me it was making him feel worse and asked me to leave him alone about it.
Instead of documenting the refusal and moving on, I came back an hour later when things had calmed down and asked if he'd be willing to tell me more about what he was experiencing. He said every time he stood up, he got so dizzy he thought he was going to fall.
Nobody had explained to him that orthostatic hypotension is a common side effect and something we could manage with positioning changes and timing. Once I walked him through it and gave him a concrete plan — sit at the edge of the bed for a minute before standing, always use the call button before getting up — his whole attitude shifted. He took his medication that day and every day after.
I flagged the conversation to the charge nurse and documented it because it was directly relevant to his discharge teaching and safety plan. Before he left, he thanked me. I didn't expect that."
What makes this answer work: It shows clinical knowledge (orthostatic hypotension as a real side effect), patient advocacy (going back rather than just documenting the refusal), communication skills, documentation, and a genuinely human moment at the end. The result is specific, not vague.
"Describe a conflict you had with a coworker and how you resolved it."
Hiring managers ask this to find out if you're the kind of person who avoids conflict, escalates it unnecessarily, or handles it like a professional adult. They've seen all three.
The strongest answers show that you addressed the issue directly and privately — not through gossip, not by going above the person's head unless you had to, and not by pretending it didn't happen.
"About six months into my first job, I noticed that one of my coworkers was consistently giving me incomplete handoffs — leaving out pending labs, changes in condition, or family concerns that had come up during her shift. I initially assumed it was unintentional, but after it happened several times, I knew I needed to address it.
I asked if we could talk privately before our shifts overlapped one day. I was direct but not accusatory — I told her I'd noticed some gaps in handoff and that I wanted to find a way to make sure we were both set up for a safe shift. I framed it around patient safety rather than making it about her.
She told me she'd been under a lot of personal stress and had been rushing through the end of her shifts. We agreed on a quick checklist format for handoff that we both used going forward. The incomplete handoffs stopped.
I didn't go to the charge nurse about it beforehand because I felt like I owed it to her to address it directly first. If it had continued after that conversation, I would have involved our supervisor — because at that point it would have been a patient safety issue, not just a communication preference."
What makes this answer work: It addresses the issue directly, shows professional maturity, frames the concern around patient safety (not personal frustration), and explicitly names what the escalation path would have been. That last part is important — it shows you understand when direct resolution is appropriate and when it isn't.
"Tell me about a time you made a mistake."
This is one of the questions nurses dread most — and the one that separates honest, self-aware candidates from the rest.
A few rules: the mistake needs to be real. "I can't think of one" is a red flag. Minimizing the mistake by subtly blaming the situation is also a flag. And picking a mistake that's clearly not a mistake ("I worked too hard and had to slow down") insults the interviewer's intelligence.
Pick something real, own it clearly, and end with the specific thing you changed.
"During my clinical rotation, I was caring for a patient who had just come back from a procedure. She mentioned she felt nauseous, and I noted it but didn't follow up as quickly as I should have — I got pulled into another room and assumed it was routine post-procedure nausea that would pass.
About an hour later, one of the staff nurses noticed the patient hadn't moved much and her coloring wasn't great. We reassessed together and found her blood pressure had dropped. She ended up being fine, but it required intervention that could have happened sooner if I had taken her symptom more seriously and done a full reassessment at that point.
What I changed after that shift: I now do a focused reassessment any time a patient reports a new symptom, even a vague one. I write it on my assignment sheet so I don't rely on remembering it while I'm managing other patients. 'I'll come back to that' without a specific plan is not a safe approach."
Why this answer works: It names a real clinical gap — underweighting a symptom — without catastrophizing. It owns the mistake without blaming the situation. And the behavioral change at the end is specific and believable, not a vague "I'll pay more attention."
"Tell me about a time you had to prioritize multiple patients at once."
Every nurse gets this question. The answer that fails: "I just stayed calm and worked through my list." The answer that works: a specific example with clear reasoning behind each decision.
"During a busy night shift on my med-surg rotation, I was helping cover for a nurse who had called in. I had four patients, and within the first hour, two of them needed attention at the same time.
One patient had a pain rating of 8 out of 10 and was asking for her scheduled pain medication, which was due. The other had just been helped back to bed by a tech and his call light was on — when I answered, he said he felt short of breath.
I told the patient waiting for pain medication that I would be with her as soon as I safely could and that I was responding to another patient. Then I went directly to the patient reporting shortness of breath — that was a new symptom that needed an assessment, not just reassurance.
I checked his oxygen saturation and respiratory rate, which were both within normal range, but he was anxious and his respirations were slightly shallow. I repositioned him, put him on a couple of liters of supplemental oxygen per standing orders, and stayed with him until he settled. Then I looped in the charge nurse before I went back to the other patient, so she knew what was happening and could have eyes on him.
I got the pain medication to the first patient about 12 minutes after she asked. I apologized for the delay and explained that another patient had needed immediate attention. She was understanding."
Why this answer works: It shows clear clinical prioritization — a new symptom over a scheduled medication, even though both mattered. It shows communication with the charge nurse. And the brief interaction with the first patient at the end shows professionalism and basic patient communication, which interviewers notice.
"Tell me about a time you advocated for a patient."
This is a question about moral courage as much as clinical skill. The best answers involve a real moment where advocating for the patient required you to speak up, push back, or escalate something when it would have been easier to stay quiet.
"During my cardiac rotation, I had an elderly patient who was being prepared for discharge the following morning. Her daughter, who was her primary caregiver, hadn't been in and wasn't aware of the discharge plan. When I asked the care team about family notification, I was told it had been addressed — but when I called the daughter myself to do discharge teaching, she had no idea her mother was going home the next day and had not arranged any support at home.
The patient had moderate dementia and was not going to be able to manage her medication changes independently. Sending her home without a plan in place felt unsafe.
I brought this to the charge nurse and the attending. I documented specifically what the daughter had told me and what the home situation looked like based on the patient's history. The discharge was delayed by 24 hours to allow for a proper care conference and home health arrangements.
The patient's daughter was relieved. The attending was frustrated with the delay, but acknowledged in the chart that the revised discharge plan was more appropriate. What I took from that situation: discharge safety is not just about whether the patient is medically stable. It's about whether there's a safe environment for them to go to."
Why this answer works: It shows genuine advocacy — not just a vague desire to "help patients," but a specific action that required speaking up against pressure. The result was inconvenient but clinically sound. The lesson at the end shows mature thinking about what discharge safety actually means.
Preparing Your Own STAR Stories
The model answers above are examples. Your answers need to come from your own experience — your own clinical rotations, your own floor moments, your own mistakes.
Here's a practical way to prepare:
Write down five to seven clinical moments before the interview. These should be specific enough that you can recall the setting, the patient situation, and what you specifically did. They don't need to be dramatic. A moment where you caught a medication discrepancy during handoff is a perfectly usable story.
For each moment, map it to STAR. Write one to two sentences for Situation, one sentence for Task, three to five sentences for Action, and one to two sentences for Result. Keep the Action step the longest.
Practice each answer out loud, not just in your head. Record yourself if it helps. Your goal is 60 to 90 seconds per answer — clean, specific, and ending on a result.
Use the same stories for multiple questions. One good clinical story can answer "tell me about a time you showed clinical judgment," "tell me about a time you worked under pressure," and "tell me about a time you communicated with a physician" depending on how you emphasize different parts. You don't need a different story for every possible question — you need five good stories you know well.
A Note on SBAR and When It Fits Into Your STAR Answer
SBAR — Situation, Background, Assessment, Recommendation — is the standard communication framework used in clinical escalations. It's different from STAR, but the two frameworks often appear together in nursing interview answers.
If your STAR story involves calling a physician, escalating a concern to a charge nurse, or handing off a patient, the Action step of your answer should reflect SBAR communication. You don't need to name SBAR out loud — just structure your description of the call or conversation in that order: what you were calling about, the relevant background, your assessment of the situation, and what you asked for.
When an interviewer who works in clinical care hears that structure in your answer, they recognize it. It signals that you communicate the way experienced nurses communicate, even if you haven't been doing it for long.
For a deeper look at how SBAR works in clinical scenario questions — including the physician disagreement question and rapid deterioration scenarios — see ICU Nursing Interview Questions and 50 Nursing Interview Questions and Answers.
The Bottom Line
The STAR method is a tool, not a script. Knowing the letters is not enough.
What makes a nursing behavioral answer strong is the Action step showing real clinical thinking — that you prioritized the right things, communicated with the right people, and kept the patient at the center of every decision.
Prepare five real stories from your clinical experience. Practice them out loud. Keep your Situation brief, your Action specific, and your Result honest.
The nurses who stand out in behavioral interviews are not the ones with the most dramatic stories. They're the ones who can tell a simple, real story clearly — and who can explain exactly what they did and why.
Practice your STAR answers before the interview.
Vorna gives you real nursing behavioral questions based on your resume and the role you're applying for — then scores your answers on STAR structure, clinical reasoning, and communication. Free to start.
For a full list of behavioral and clinical questions — with model answers — read 50 Nursing Interview Questions and Answers →
New grad? New Grad Nursing Interview Tips covers how to answer behavioral questions when your clinical experience is still limited.